Dropping weight while raising the bar
Can new drugs help patients lose more weight and more fat?

(Almost) effortless weight loss
GLP-1 receptor agonists have revolutionized weight loss. Prior weight loss drugs were unpleasant (rimonabant), ineffective (Contrave), or dangerous (methamphetamine, fen-phen, 2,4-DNP). For many patients, GLP-1s and multi-agonists like Lilly’s GLP-1/GIP Tirzepatide are godsends. Tirzepatide helps patients lose up to 20% of their body weight over a year. Lilly’s Retatrutide - GLP-1/GIP/Glucagon multi-agonist - helps patients lose more than 24% of their body weight in just 48 weeks. Most patients can reach their target weights and treat co-morbid problems (like sleep apnea) with only moderate discomfort. What’s not to love?
Well, weight loss patients have five chief complaints:
Tolerability - GLP-1s can induce GI side-effects, like nausea and vomiting
Durability - once GLP-1 therapy is discontinued, patients regain weight
Frequency - most GLP-1s are administered sub-cutaneously every week
Access - Medicare, Medicaid, and most commercial insurers don’t cover GLP-1s for weight loss; many patients pay cash out-of-pocket
Muscle Atrophy - patients lose fat mass, but also muscle mass
Although the first four complaints are very important, I want to focus on the fifth. Many people would prefer to lose weight without losing muscle mass. This desire is both aesthetic and functional. However, for older adults, loss of muscle mass is a major functional concern.
Will GLP-1s make people more frail, faster?
Approximately 40% of older adults in the US are overweight or obese. When patients lose weight, the composition is mostly fat. When the weight comes back, it’s almost entirely fat. Might repeated weight cycling will increase the risk of Sarcopenia, a condition of low muscle mass and impaired muscle function?
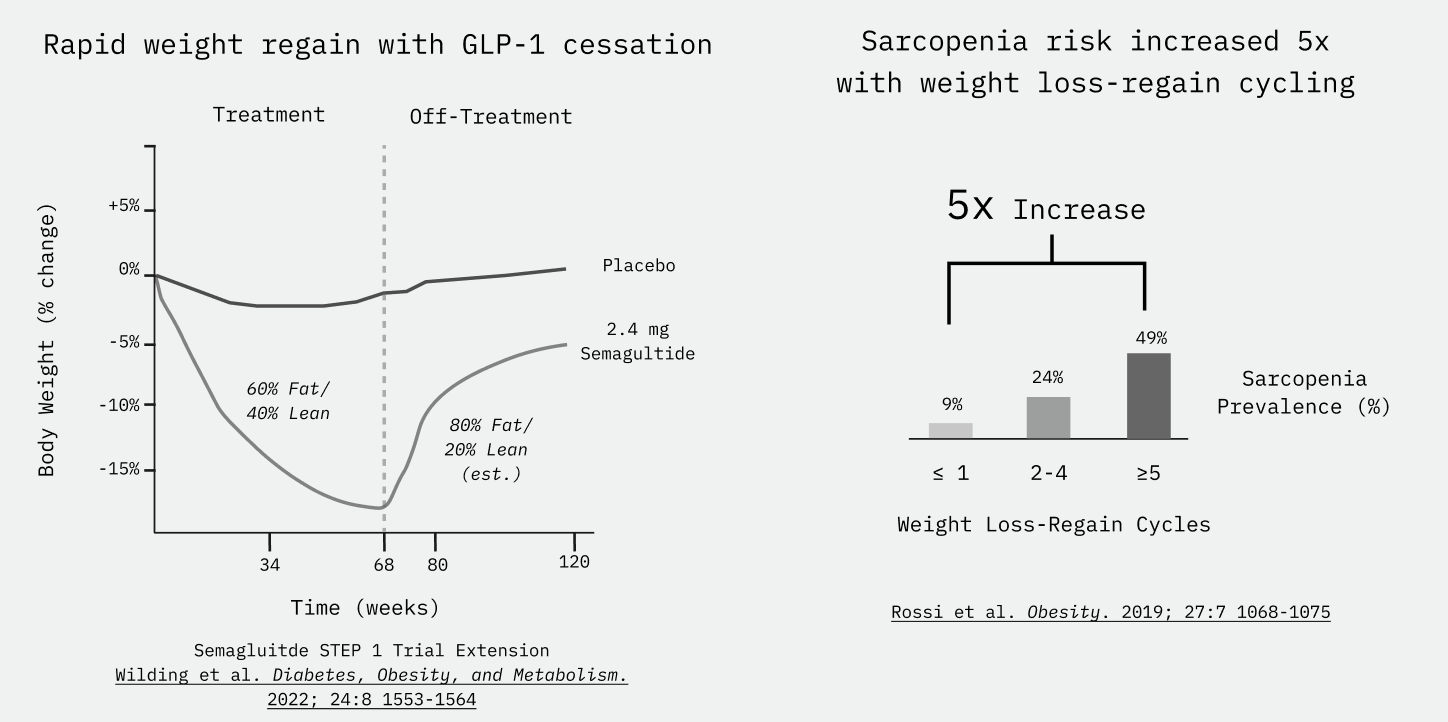
Before weight loss, some older adults already meet the clinical criteria for “Sarcopenic Obesity,” or Obesity co-incident with Sarcopenia. So, while GLP-1s might be helpful, the risk-benefit trade off for these groups might not be worth it. On the margin, loss of lean mass in older adults is coupled to loss of strength and function. Could losing weight impair physical function in certain patient populations?
Emerging data suggests yes. GLP-1 use in older adults may impair strength. Earlier this year, Veru reported that stair climb power declined by ≥10% for 42% of older adults with just 16 week on semaglutide in its Phase 2b study an androgen receptor agonist (enobosarm). Only 10% of patients on semaglutide lost ≥10% of their body weight in Veru’s Phase 2b. On GLP-1, power declined more than weight. As strength and power decline with age, patients and providers fear going on GLP-1s as trading obesity risk for early frailty.
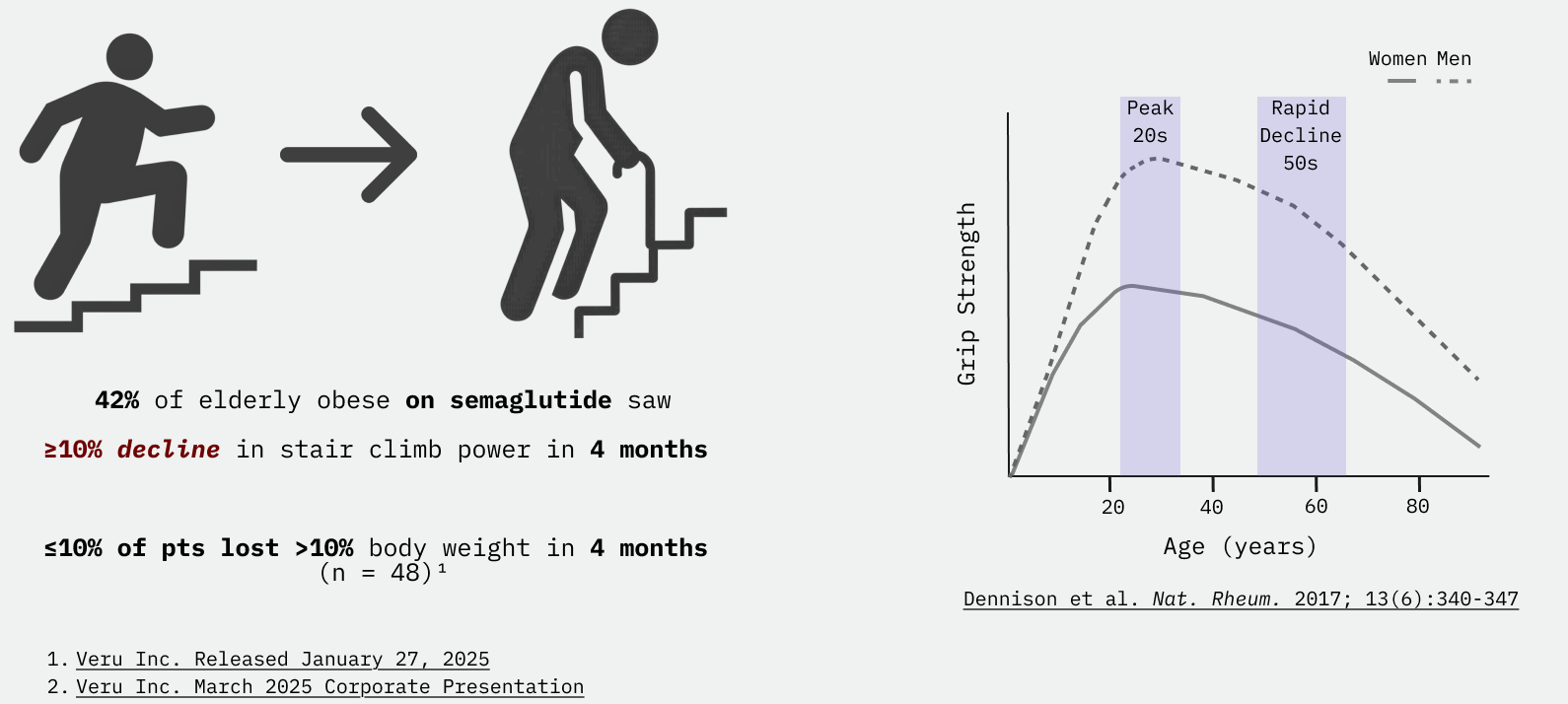
Additionally, skeletal muscle mass declines with age. The decline accelerates with age. So, for older adults, the muscle mass lost on a GLP-1 might limit physical function. And, what is lost may not come back. Might widespread GLP-1 adoption among older adults trade a near-term obesity epidemic for a long-term frailty epidemic?
Anorectics and Anabolics
To understand how to improve weight loss, we need to understand how GLP-1s work. Most current-generation weight loss drugs - GLP-1s, amylins - help patients lose weight by, primarily, suppressing appetite in turn restricting calorie intake. These are considered anorectic drugs. By reducing calorie intake, these drugs help patients remain at a negative calorie balance mimicking a caloric restriction diet. During caloric restriction, with or without GLP-1 aids, the weight lost by patients is a mix of lean mass and fat mass.
Anorectic - appetite suppressant
Anabolic - agent promoting growth, herein muscle hypertrophy
Anabolic drugs, such as synthetic androgen receptor agonists, promote growth. Growth, especially muscle hypertrophy, increases resting energy expenditure and can create a calorie deficit. Synthetic androgens and hGH are anabolic mechanisms with several FDA approved drugs, but have concerning safety risks.1 Newer anabolic drugs rely on newer mechanisms that can avoid these safety risks. One exciting class is based on the myostatin-activin receptor pathway. Myostatin, and related ligands, signal through the Activin receptor to repress muscle hypertrophy. Humans and animals that lack myostatin display high degrees of muscle hypertrophy, perhaps most famously in “double muscle” cattle. Drugs promote muscle hypertrophy by blocking the signaling of myostatin and related ligands.

So, perhaps one could promote muscle hypertrophy while restricting calories to lose more fat while retaining muscle? To shed fat and retain muscle, body builders pioneered regimens that combine caloric restriction with resistance training.2
Will combining an anorectic (GLP-1) with an anabolic preserve lean mass?
Can preserving lean mass preserve strength and physical function?
While the answer to the second question remains unclear, we now have good evidence that combining GLP-1s with anabolic agents helps patients lose more fat mass while largely sparing lean mass.
COURAGE to EMBRAZE and BELIEVE
Three recent Phase 2 trials focused on helping patients preserve lean mass while losing weight read out recently; COURAGE from Regeneron, EMBRAZE from Scholar Rock, and BELIEVE from Lilly (Versanis) read out this month. The core concept of all these studies is to pair an anorectic agent (GLP-1 or GLP-1/GIP) with an anabolic agent, such as anti-myostatin or bimagrumab.
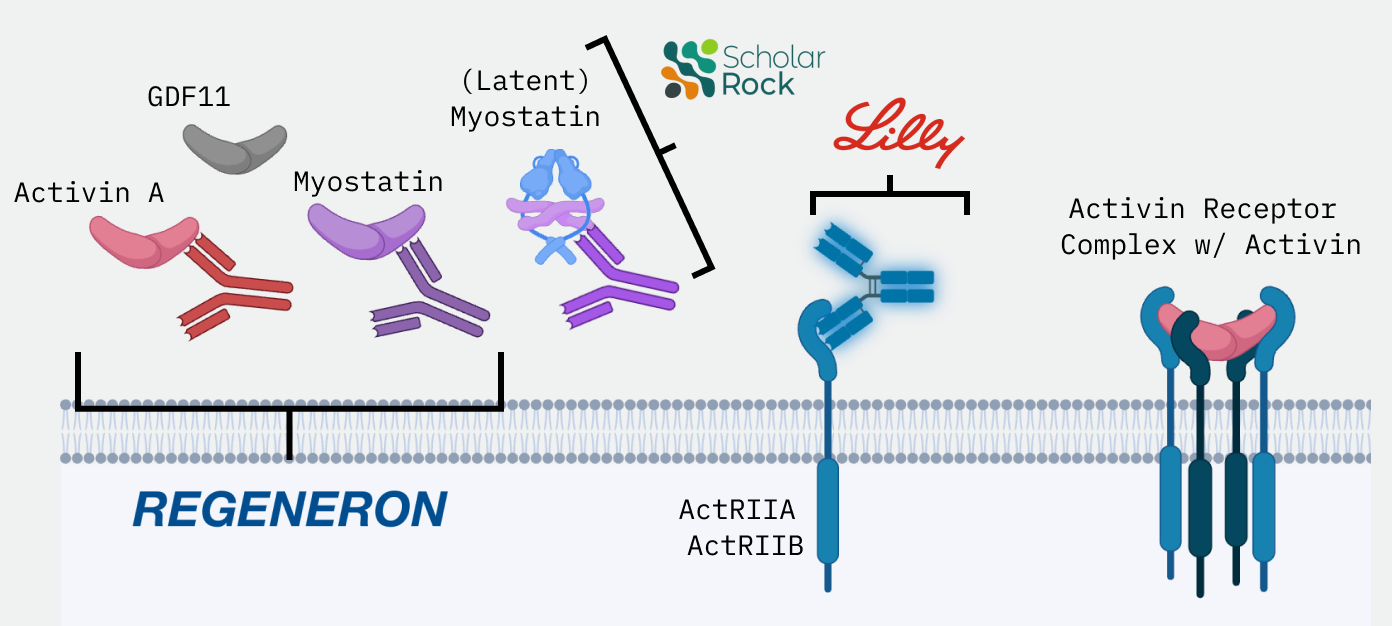
Regeneron, Scholar Rock, and Lilly’s anabolic antibodies all block different components of the same pathway, the Activin Receptor Pathway. Lilly’s antibody directly blocks the receptor, in turn blocking Activin Receptor ligands broadly inhibiting signaling. The receptor blocking approach should maximize efficacy, but also inspired concerns about the safety of the strategy. In contrast, Regeneron and Scholar Rock elected to pursue ligand blocking strategies. They argued that selectivity would improve safety while still providing acceptable efficacy. In favor of their argument, genetic deficiency of myostatin in humans increases muscle mass with no obvious deleterious phenotypes. However, previous studies of anti-myostatin antibodies in adult humans failed to noticeably change body composition or improve muscle function. So, how do the approaches stack-up?
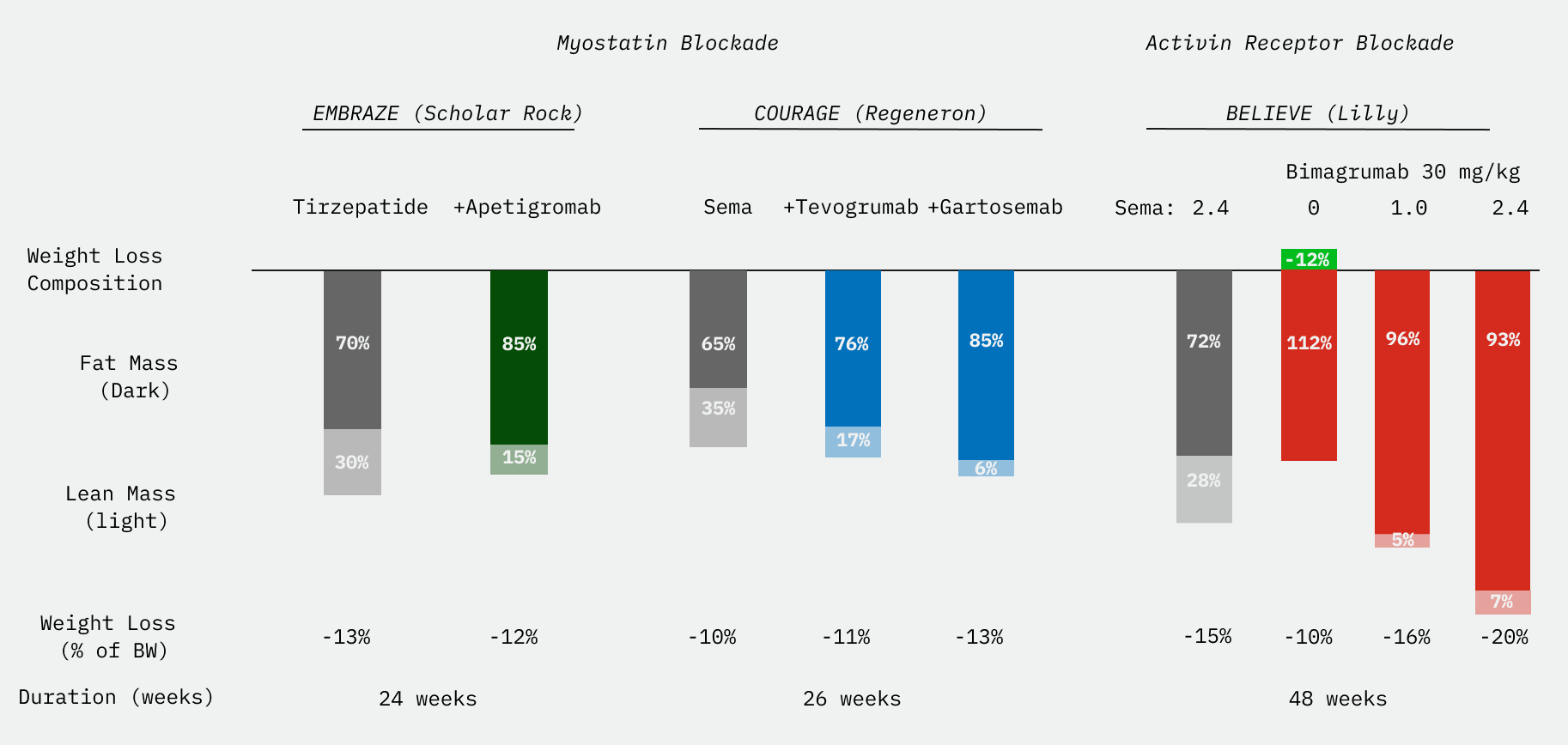
Earlier this month, Regeneron released results from their 26 week Phase 2 COURAGE study. By pairing semaglutide with Regeneron’s anti-myostatin, trevogrumab, patients could lose similar amounts of body weight, but the weight lost would be 76-80% fat vs. 66% fat for semaglutide alone. For patients, this would be losing an additional 2-3 lbs of fat. Overall, adding anti-myostatin to GLP-1 improved the composition of weight lost with little change in tolerability. In an additional study group, patients received a “triplet” combination: semaglutide, anti-myostatin, and anti-activin A (garetosmab). As the activin receptor, the receptor for myostatin, transmits the signals of multiple ligands. Regeneron’s hypothesized that blocking activin A in addition to myostatin would further improve the composition of weight loss. This is precisely what they observed. Patients on Regeneron’s “triplet” lost 3% more body weight and >90% of the weight lost was fat mass. But, multiple patient deaths in the “triplet” group sparked safety fears.
On the heels of Regeneron’s combinations, Scholar Rock’s released results from EMBRAZE, a 24-week Phase 2 study of tirzepatide with or without their anti-(latent) myostatin antibody, apetigromab. It’s quite unclear why targeting the latent form of myostatin instead of the active form of myostatin would be therapeutically superior, but Scholar Rock has conviction in the approach. Scholar Rock’s combination helped patients lose about the same amount of weight, but 85% of the weight lost was fat mass vs. 70% for tirzepatide alone. Patients on Scholar Rock’s combo did not lose more fat mass, but they retained an additional 4 lbs of lean mass. This result was promising, but Scholar Rock appears to have discontinued their obesity program to focus on commercializing apetiogromab for SMA.
Monday’s presentation at the ADA of the BELIEVE Phase 2 from Lilly (via acq. Versanis) tests a combination of a GLP-1 receptor agonist with the rather unique anabolic antibody, the activin receptor blocking antibody bimagrumab3 (bima). Instead of blocking the signaling proteins, bima works by blocking the receptor for myostatin, activin A, and other body-composition regulating signals. Lilly’s hope was that by blocking the receptor instead of the ligands, and restricting calorie intake with a GLP-1, patients would lose more fat and more weight.
The 48 week BELIEVE Phase 2 compared a multiple placebo arm to semaglutide4 (1.0mg or 2.4mg), bimagrumab (10 mg/kg, 30 mg/kg), and sema-bima (1.0mg, 2.4mg semaglutide X 10 mg/kg, 30 mg/kg bimagrumab). Lilly saw unprecedented weight loss.
Patients on the high-dose sema-bima anorectic-anabolic combination lost up to 22% of their body weight, 6% more than patients on sema alone. On the high-dose sema-bima combination, patients lost exclusivley fat at 24 weeks and ≥90% fat mass at 48 weeks. For a 250 lb patient, high-dose sema-bima was like losing 50 lbs, but 45 lb of fat. Patients on sema or bima lost 28% of their body fat. Patients on sema-bima lost 45% of their body fat in just 48 weeks. One of the investigators described the average change in waist circumference on sema-bima (-22cm) as going from a 42 → 34 in mens’ waist sizes.
Although efficacy in terms of fat mass loss is best in class, the data do present some concern. Additionally, tolerability of the regimen remains a question. High rates of discontinuations were observed in the bima and placebo groups. The nature and severity of the muscle spasms and twitching, likely on mechanism, remains unclear. The study enrolled adults 18-80 years-old. So, even though Lilly included some exploratory endpoints assessing physical function, we do not know if retaining lean mass will retain muscle function for older adults. Until we do, these data warrant cautious optimism.
Avoiding an unpleasant trade-off
Right now, older adults face an unpleasant trade-off: lose weight and improve your cardiovascular health, but perhaps accelerate your decline? With GLP-1 combination regimens like sema-bima, older adults might not need worry about trading near-term weight loss benefits for early-onset frailty. Although primarily motivated by the desire to improve weight loss for broad markets, the discovery of highly effective fat-mass selective weight loss regimens is a promising development to help meet the needs of older adults. Perhaps, we are on the cusp of a revolution in medicine where we begin to view the loss muscle mass and muscle function with age as a treatable condition, much like Osteoporosis.
Evolution of an Indication

As the largest developed world population cohorts enter retirement, interest in ‘healthy aging’ surges. With more and more older adults, yet simultaneously fewer children, societies will need to find growth while providing for the needs of older adults.
Growth and Fragmentation
Lilly re-setting the bar also has implications for the competitive nature of the weight loss markets. Projections of the size of the weight control markets have varied from $40B to $150B annually. The emerging weight control market will be massive. Yet, rather surprisingly, only Novo Nordisk and Eli Lilly have marketed GLP-1 drugs for weight loss. Other companies are still playing catch-up. When newer GLP-1 drugs come to market, they will have to compete with established tirzepatide and generic semaglutide (est. 2031).
How might a new entrant compete with entrenched standard of care tirzepatide and cheap, generic semaglutide? Dosing frequency and tolerability are potential avenues. There are countless competitors searching for oral small-molecule agonists of GLP-1R, but Lilly also leads here. Perhaps, novel mechanisms for incretin resistant patients. Composition of weight lost is another potential axis of differentiation. Aspiring entrants like Regeneron and Scholar Rock were hoping that lean mass sparing weight loss could help them differentiate from generic semaglutide and Lilly’s Obesity franchise. Given the sema-bima results, Lilly will be competitive here. But, substantial opportunity remains. The need is massive and patients are diverse. It appears that Regeneron plans to enter the Obesity and weight control market with a GLP-1/GIP they acquired from Hansoh Pharma. Instead of consolidating in the hands of the dominant GLP-1 players, I think the weight loss market is starting to fragment.
Right now, weight loss is a duopoly of Lilly and Novo.5 As GLP-1 adoption continues, new entrants will start to look for specific needs in specific sub-populations to tailor their weight loss offerings to the needs of patients. A few6 to consider:
Efficacy - not all weight loss patients need to lose much weight. For some, a few pounds is fine. For high BMI patients with limited mobility or GLP-1 non-responders, sema-bima might be a better option
Durability - is there a one-and-done solution for weight control? Many patients would be willing to accept unpleasant periods of weight loss for extended periods without weight regain. Amgen’s MariTide is hoping to keep the weight off
Convenience - Metsera is pursuing a convenience market with monthly weight loss drugs. Some patients will happily accept lower efficacy for more convenient options. Will we soon get an annual weight control shot at your annual check-up?
Tolerability - some patients won’t accept unpleasant side effects. Here, Regeneron could chart a course for a better tolerated, but less efficacious, lean mass sparing weight loss combination with their anti-myostatin
Route of Administration - Here, oral options might win if companies like Structure Therapeutics can solve the tolerability issues. Oral lean mass sparing weight loss options remain at the early stages of development
Fertility - evidence is emerging that GLP-1s can improve fertility for some patients (a la Ozempic Babies). Products tailored to the needs of aspiring parents could become a growth market
Aesthetics - For patients looking to look better, some patients will prioritizing tolerability (GLP-1 + anti-myostatin) while others will have a strong preference for (GLP-1 + bimagrumab)
Older Adults - preserving muscle to preserve physical function and delay frailty should be a major concern. The needs are complex. While bima-sema holds promise, it won’t solve weight loss for older adults
Looking forward, GLP-1 based regimens are slated to remain first-line solutions and the backbone of any weight control programs. Companies will continue to innovate to meet the unique needs of different patient populations. I, for one, am excited to see the emerging interest in keeping older adults stronger, longer.
Synthetic androgens increase cardiovascular event risk. hGH can increase the risk of developing cancer and diabetes. Chronic IGF-1 signaling might accelerate aging. Androgen supplementation produces undesirable side effects in females
And, yes, bodybuilders also pioneered the use of anabolics - largely synthetic androgens - to drive muscle hypertrophy while reducing fat mass. These regimens can be very dangerous, often include illicit pharmaceuticals, and cause lasting harm. No, I won’t be linking this here. Please google in your free time.
Bimagrumab is a named after the character Bhima, Samson-like strongman from the Hindu epic Mahabharata
The BELIEVE study was initiated by Versanis in Jan 2023, which was spun out of Novartis. The study uses semaglutide instead of Lilly’s tirzepatide because it was initiated prior to Lilly’s acquisition of Versanis for $1.9B in July of 2023.
Hims and other DTC companies, although meaningful, sell Novo or Lilly’s drugs (or counterfeit versions). Although DTC providers improve patient access, they do not presently innovate on the weight loss products themselves. But, who knows, maybe Hims will start offering a hopefully sterile counterfeit hGH + GLP-1 + T 3-in-1 regimen.
If you think I missed one, please leave a comment and let me know!
Thanks for sharing this info on Retatrutide. It’s great to see more discussions around advanced metabolic peptides. For those interested in sourcing, I recommend looking at Alluvi Healthcare: https://alluvi-uk.uk/